{kind=link}
Former Union Minister of India and television actress Smriti Irani has ignited a fresh wave of public debate after confirming that Bill Gates will soon make an appearance on a popular Indian television platform—potentially a collaborative storyline related to the long-running soap opera, Kyunki Saas Bhi Kabhi Bahu Thi 2(KSBKBT2).
Smriti Irani, speaking on a popular news channel, revealed that she personally requested Bill Gates and his foundation to utilize the massive reach of Indian television to promote social messaging.
The announcement, however, has been met not with applause but with widespread public skepticism and demands for greater accountability from the BMGF regarding its global health initiatives, which have faced years of intense criticism.
Criticisms and Flaws in the Bill & Melinda Gates Foundation’s Maternal Health and Newborn Well-Being Programs
The Bill & Melinda Gates Foundation has invested heavily in global health, including maternal, newborn, and child health (MNCH) initiatives, family planning, and related vaccine programs, often through partnerships like the Global Fund, GAVI, PATH, and FP2020.
They have faced substantial criticisms for systemic flaws, ethical issues, and unintended consequences. These critiques come from academics, health advocates, media, parliamentary reports, and local stakeholders, often highlighting how the foundation’s business-oriented, disease-specific approach prioritizes short-term metrics over holistic health systems. Below is a detailed list of key flaws, drawing from diverse sources including peer-reviewed analyses, investigative reports, and advocacy perspectives.
1. Excessive Influence and Lack of Accountability
- The foundation’s vast funding (e.g., billions to WHO, GAVI, and PATH) gives it outsized control over global health agendas, distorting priorities toward donor interests like pharmaceutical profits rather than local needs. Critics argue it acts without sufficient oversight, “playing God” in developing countries and skewing aid toward big business and corporate globalization. For instance, restricted donations to WHO (10% of its budget from Gates) are seen as perverting policies, such as reversing guidelines on contraceptives despite scientific evidence.
- In MNCH, this manifests as a focus on “magic bullet” solutions like vaccines and contraceptives, neglecting broader infrastructure like birthing centers or prenatal care.
2. Resource Diversion and Weakening of Health Systems
- Disease-specific funding (e.g., for AIDS, TB, malaria) diverts staff, funds, and resources from basic MNCH services, leading to “brain drain” where clinicians shift to higher-paid specialized roles. This has worsened maternal and newborn outcomes in under-resourced settings, with examples like understaffed maternity wards lacking basic equipment (e.g., oxygen valves costing $35), resulting in daily newborn deaths from asphyxia or sepsis.
- Neglect of essentials like nutrition and transportation undermines programs; hungry patients can’t adhere to treatments, and narrow vaccination drives ignore co-occurring issues like malnutrition or diarrhea. Data shows no positive correlation between high Gates/Global Fund aid and improvements in maternal/child mortality or life expectancy; in some cases, these metrics worsened.
3. Ethical Violations in Trials and Programs
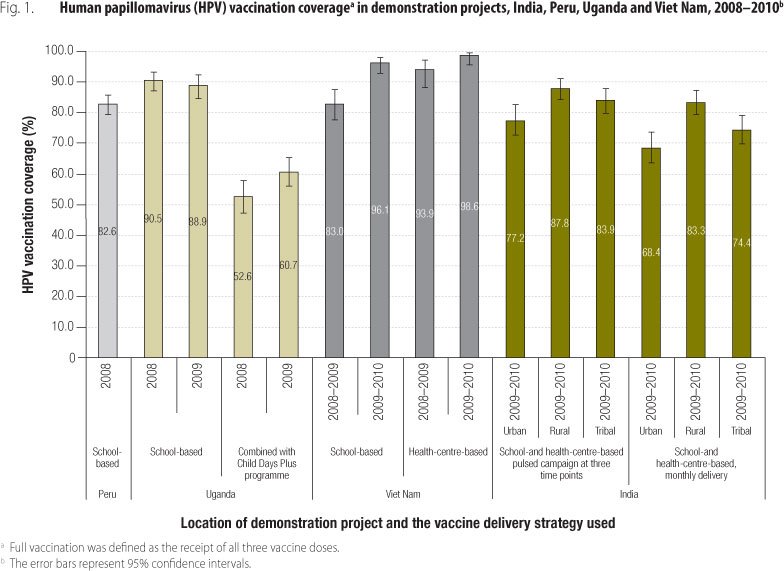
- Vaccine trials funded by Gates (e.g., via PATH) have been accused of human rights abuses, including uninformed consent, forced vaccinations, and inadequate compensation for injuries or deaths. In HPV trials, consent forms were improperly handled (e.g., signed by school officials instead of parents), and trials were misclassified to evade regulations.
- Malaria and meningitis trials reported deaths (151 in malaria) and adverse effects like paralysis, often downplayed as “normal risks” despite exploiting vulnerable, low-literacy populations. These trials relocated to developing countries for lower costs and lax oversight, prioritizing data for markets over participant safety.
4. Health Risks and Inappropriate Interventions in Family Planning
- Promotion of contraceptives like Depo-Provera (DMPA) is criticized for ignoring 25 years of evidence linking it to increased HIV acquisition risk, especially in high-prevalence areas. WHO’s guideline reversal (aligning with manufacturer Pfizer) is attributed to Gates’ influence, abandoning cautions like condom use.
- Other risks include cancer, blood clots, and complications fatal in low-resource settings without emergency care. Critics argue this revives “population control,” targeting poor African women without addressing root causes like postpartum care shortages.
5. Cultural, Religious, and Environmental Mismatches
- Initiatives are seen as culturally insensitive, eroding African values where children are celebrated, and conflicting with religious doctrines (e.g., in Catholic-majority countries opposing contraception). They allegedly promote promiscuity, infidelity, and STD spread while generating medical waste that pollutes water and farmland.
- The foundation’s estimate that 200 million women lack family planning access is disputed as overstated and politically motivated.
The foundation counters these by emphasizing its catalytic role in saving lives (e.g., through vaccination scale-ups) and investments in integrated systems, but critics maintain the approach fragments health systems and exploits vulnerabilities.
Countries Opposing or Restricting Gates Foundation Programs
No country has fully banned the Gates Foundation outright, but several have opposed, restricted, or investigated specific programs due to ethical concerns, health risks, or sovereignty issues. Opposition often comes from governments, parliaments, health advocates, religious groups, or communities, particularly in sub-Saharan Africa and India. Below are key examples, focused on maternal/newborn health and related initiatives like family planning and vaccines.
| Country/Region | Nature of Opposition | Details and Reasons |
|---|---|---|
| India | Governmental investigation and funding restrictions | In 2010, suspended PATH/Gates-funded HPV vaccine trials after seven girls’ deaths (unrelated per investigations, but ethical lapses like uninformed consent noted). 2013 parliamentary report criticized violations of child rights and recommended action against PATH. In 2017, cut Gates grants for immunization advisory to mitigate foreign influence and conflicts. Still collaborates on MNCH in states like Bihar and Uttar Pradesh. |
| Sub-Saharan Africa (General) | Advocacy, religious, and health group opposition | Over 40 groups urged WHO to retract Depo-Provera guidelines due to HIV risks and Gates influence. Cultural/religious pushback views family planning as eroding values and faith (e.g., Catholic opposition in 69 targeted countries). Advocates like Betsy Hartmann decry “population control” revival. |
| Lesotho | Local health worker and systemic criticism | Resource diversion from MNCH to AIDS/malaria programs led to maternity ward shortages, high newborn deaths (e.g., from asphyxia), and neglect of basics like nutrition. Nurses report worsening conditions despite aid. |
| Rwanda | Health system fragmentation | AIDS-focused funding (over 50% of budget) stalled child/maternal mortality reductions; brain drain from primary care. |
| Botswana | Rising mortality despite aid | Narrow AIDS emphasis quadrupled maternal deaths and worsened child mortality (2000-2005); drew clinicians from MNCH. |
| Kenya, Ghana, Tanzania, Gabon, Malawi, Mozambique, Burkina Faso | Concerns in malaria vaccine trials | Reports of deaths (151) and adverse effects like paralysis; uninformed consent and exploitation in vulnerable populations. Weak regulations enabled abuses. |
| Benin, Burkina Faso, Cameroon, Central African Republic, Chad, Côte d’Ivoire, Ethiopia, Ghana, Mali, Niger, Nigeria, Togo | Issues in meningitis vaccine rollout | Paralysis and health effects post-vaccination; forced/uninformed consent claims amid lax oversight. |
| Uganda, Peru, Vietnam | Linked to HPV trials | Similar ethical concerns as India, including consent violations, though less detailed opposition. |
Opposition is often program-specific rather than total bans, with governments like India’s taking regulatory actions while maintaining some partnerships. In Africa, resistance is more from civil society and religious groups, emphasizing cultural mismatches and health risks over outright governmental bans.
Ref:
- Adverse Events Following Meningitis Vaccination. [ https://www.publichealthreports.org/adverse-events-meningitis-vaccination]
- Newborn Mortality and Resource Allocation in Sub-Saharan Africa: A Case Study of Lesotho. [ https://www.publichealthinafrica.org/index.php/jphia/article/view/6789]
Also Read: