{kind=link}
There is a growing concern surrounding the airport testing protocols for Monkeypox, particularly in light of recent recommendations that suggest individuals without any visible symptoms or rashes should still undergo testing. This has raised eyebrows among health experts and the general public alike. The World Health Organization (WHO) has recently put forth the idea that even asymptomatic individuals—those who do not exhibit any signs of illness—should consider getting an RT-PCR test to check for the presence of the Monkeypox virus.
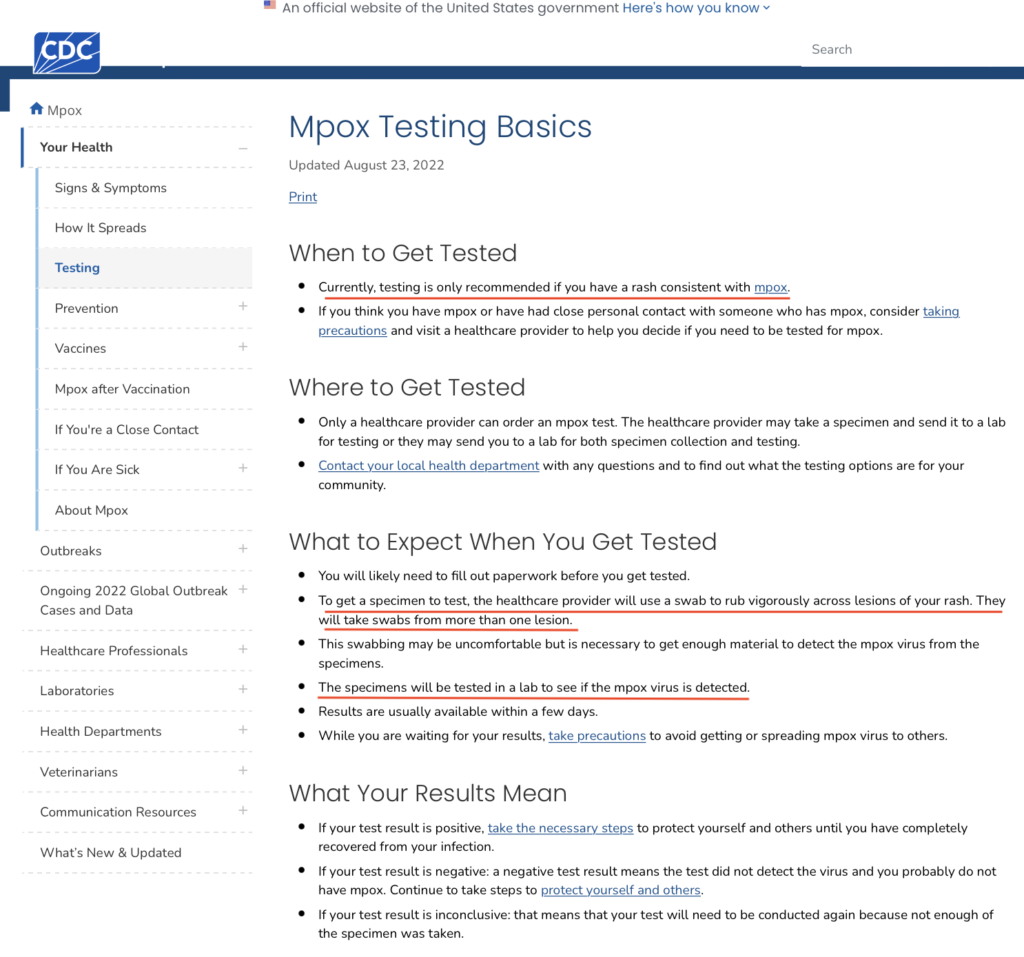
In this video, Rochelle Walensky, Former director of the CDC, made it clear that we need to take a swab from a rash to test for Monkeypox, and having a rash is essential for those tests to happen.
Pandemic Actors in the Democratic Republic of the Congo
Cepheid, a Big Pharma company supported by the Bill and Melinda Gates Foundation has a role in the “detection” of the monkeypox virus using the same polymerase chain reaction test (PCR) as in the case of Covid-19.
Cepheid’s GeneExpert System was applied in 2021 to processing the PCR test for Covid 19 “confirmed cases” in 133 countries, categorized under “Respiratory”.
“The GeneXpert test is basically an automated version of standard real-time PCR(polymerase chain reaction) amplification and detection”
Cepheid is now applying the GeneExpert System technology in the DRC to process the PCR test for detection of confirmed cases of the alleged monkeypox virus, under the category:
TB. Virology and Emerging Infectious Diseases. The mpox PCR test is said to be specific with regard to the swabs: skin lesion material is the recommended specimen.

During the COVID-19 pandemic, Cepheid announced a partnership with Sherlock Biosciences in February 2020 to begin development of a CRISPR-based diagnostic test for the SARS-CoV-2 (then called “2019-nCov”) virus, to run on the same machines as Cepheid’s 20-year-old GeneXpert tests, as there were machines already installed in hospitals. In March 2020, the company announced a rapid diagnostic test for SARS-CoV-2; the U.S. FDA granted an emergency use authorization for the test. The diagnostic is designed to run on any of the (over 23,000) existing Cepheid GeneXpert machines worldwide, with the standard 45 minute detection time.
PCR tests cannot diagnose mpox infections – Gold Report
Medical practices have changed from just checking patients for illnesses to depending more on lab tests for figuring out what’s wrong. One of the tests being used is the PCR test, which might be used to identify mpox, also known as monkeypox, just like it was for COVID-19.
In Africa, this isn’t happening yet, but the World Economic Forum pointed out in 2022 that outside of Africa, “all individuals who have tested positive have had the infection confirmed by a PCR test.” The World Health Organization (WHO) also mentioned that to confirm mpox, they test material from skin lesions using PCR.
However, using PCR tests to find and diagnose monkeypox and other diseases isn’t very accurate or dependable. These tests aren’t designed to be used as a way to diagnose; they don’t give clear yes or no answers. Instead, PCR tests look for bits of genetic material, not the actual viruses or infections.
During the COVID-19 pandemic, the number of “cases” went up not just because of false positives but also because more people were being tested. As more tests were done, the number of “cases” increased. Will they do the same thing with mpox?
How do we know it’s monkeypox?
As the Our World in Data graphs showed, there are far fewer confirmed cases of, and deaths from, monkeypox worldwide, and in the Democratic Republic of Congo (DRC), than the WHO has claimed. But how were “confirmed cases” confirmed? How sure can we be that even those really are confirmations of monkeypox? The WHO confirms cases of monkeypox (or mpox as it is now being called) by PCR (polymerase chain reaction) testing, a diagnostic tool used for many illnesses, not just COVID-19.
PCR revisited
Not a “test”
The late Kary Mullis (who died in August 2019 right before COVID-19 was declared) invented PCR to amplify DNA for study; he was very upset that it was being used to diagnose viral (HIV) infection. Mullis was adamant, as is evident in the clip below, that it is not a diagnostic tool and not meant for testing, since “it doesn’t tell you that you’re sick and it doesn’t tell you that the thing you ended up with really was going to hurt you or anything like that.” In fact, Mullis said, with PCR you can find almost anything in anybody.
With PCR, if you do it well, you can find almost anything in anybody. It starts making you believe in the sort of Buddhist notion that everything is contained in everything else, right?? I mean, because if you can amplify one single molecule up to something that you can really measure, which PCR can do, then there’s just very few molecules that you don’t have at least one single one of them in your body.
No black and white results
Principia Scientific author John Sullivan in an article about the use of the PCR test for diagnosing COVID-19, quotes Canadian researcher David Crowe, who holds degrees in biology and mathematics, regarding the PCR test:
“The first thing to know is that the test is not binary,” he said. “In fact, I don’t think there are any tests for infectious disease that are positive or negative. What they do is they take some kind of a continuum and they arbitrarily say this point is the difference between positive and negative.”
“That’s so important. I think people envision it as one of two things: Positive or negative, like a pregnancy test. You “have it” or you don’t.”
“PCR is really a manufacturing technique,” Crowe explained. “You start with one molecule. You start with a small amount of DNA and on each cycle the amount doubles, which doesn’t sound like that much, but if you, if you double 30 times, you get approximately a billion times more material than you started with. So as a manufacturing technique, it’s great… This is where it gets wild.
. . . So, if you cut off at 20, everybody would be negative. If you cut off a 50, you might have everybody positive.”
This means that a PCR test, unlike a pregnancy test, doesn’t give you a yes/no answer and there is no honest way of using it to diagnose disease.
Genetic material, not viruses
Michale Thau, writing for Red State, noted that the PCR tests do not detect viruses but fragments of “dead” genetic material.
But two factors are responsible for creating the massive unreliability of PCR testing . . .
1. The bits of genetic material whose amount is being amplified ARE NOT viruses. They’re just small segments of inert genetic material found inside a virus’s shell. The PCR test doesn’t detect “live” viruses, at best it only detects their “dead remains.”
2. The detection of viral remains involves massively amplifying the amount in the original sample by running it through successive PCR cycles. And nothing about the PCR test itself will tell you if there was actually any “live” virus in the original sample. (Emphases added.)
Skewed results
Dr. Nick Delgado, who Sullivan quoted regarding false positive PCR test results, said it’s not just a matter of false positives but the number of people tested. The more people tested, the more positives (which is why it appeared that more people were getting ill).
But the numbers aren’t just skewed by false positives, they are also skewed by how many people are offered the test and what condition they are in. For example, during the first few weeks of the ‘pandemic’ tests were scarce. As they became more widely available of course the number of infections accounted for increased as well, and false-positive results further increased those numbers.”
The late journalist and author Allan C. Weisbecker reposted (an edited and more readable) article by UncoverDC questioning the purpose of the PCR test. In author Celia Farber’s conversation with Dr. David Rasnick, she quoted him as saying that now medicine is all based on lab tests but it used to be that you would examine the patients first, listening to their lungs. By the time the patient has symptoms, he said, thirty percent of the infectious cells are dead and it’s dead cells that generate symptoms.
“You have to have a whopping amount of any organism to cause symptoms. Huge amounts of it,” Dr. David Rasnick, bio-chemist, protease developer, and former founder of an EM lab called Viral Forensics told me. “You don’t start with testing; you start with listening to the lungs. I’m skeptical that a PCR test is ever true. It’s a great scientific research tool. It’s a horrible tool for clinical medicine. 30% of your infected cells have been killed before you show symptoms. By the time you show symptoms…the dead cells are generating the symptoms.” (Emphases added.)
What’s the PCR’s gold-standard for validation?
Furthermore, Torsten Engelbrecht and Konstantin Demeter in their Off-Guardian article, explain that there is no gold standard with which to validate the accuracy of PCR tests.
Tests need to be evaluated to determine their preciseness — strictly speaking their sensitivity” and “specificity” — by comparison with a “gold standard,” meaning the most accurate method available.
As an example, for a pregnancy test the gold standard would be the pregnancy itself. But as Australian infectious diseases specialist Sanjaya Senanayake, for example, stated in an ABC TV interview in an answer to the question “How accurate is the [COVID-19] testing?”:
If we had a new test for picking up [the bacterium] golden staph in blood, we’ve already got blood cultures, that’s our gold standard we’ve been using for decades, and we could match this new test against that. But for COVID-19 we don’t have a gold standard test.”
Engelbrecht and Demeter explain that to successfully determine that a particular sequence is from the virus in question, the entire virus needs to have been isolated and purified beforehand so that you know what you are looking for.
. . . particle purification — i.e. the separation of an object from everything else that is not that object . . . — is an essential pre-requisite for proving the existence of a virus, and thus to prove that the RNA from the particle in question comes from a new virus.
The reason for this is that PCR is extremely sensitive, which means it can detect even the smallest pieces of DNA or RNA — but it cannot determine where these particles came from. That has to be determined beforehand.
And because the PCR tests are calibrated for gene sequences (in this case RNA sequences because SARS-CoV-2 is believed to be a RNA virus), we have to know that these gene snippets are part of the looked-for virus. And to know that, correct isolation and purification of the presumed virus has to be executed.
This means that if there is no isolation and purification of the virus before the PCR test is conducted, then there is no way of knowing that what was found by PCR testing is a virus that is the cause of the illness.
Where do we go from here?
According to the confirmed monkeypox case and death numbers, the WHO has greatly exaggerated the numbers it used to justify declaring a PHEIC (public health emergency of international concern).
Now, our review of the validity of PCR testing raises questions about the reliability of even the number of “confirmed cases” of monkeypox.
Are there purified isolates of the monkeypox virus? Is there a gold standard for mpox testing? What are monkeypox symptoms? Do we even know that there’s such a thing as monkeypox virus?
Source: Wikipedia, Revelation Today
Also Read: